Electroclinical features of lateral and medial orbitofrontal epilepsy: a case series
- By Yiou Liu,
- Siyu Wang,
- Bo Hong,
- Haixiang Wang,
- Jiuluan Lin,
- Jie Shi,
- Tong Zhao,
- Jianjun Bai,
- Jia Li
- and Wenjing Zhou
Pages 759 to 767
Cite this article
- LIU, Yiou,
- WANG, Siyu,
- HONG, Bo,
- WANG, Haixiang,
- LIN, Jiuluan,
- SHI, Jie,
- ZHAO, Tong,
- BAI, Jianjun,
- LI, Jia
- and ZHOU, Wenjing,
- Liu, Yiou.,
- et al.
- Liu, Y.,
- Wang, S.,
- Hong, B.,
- Wang, H.,
- Lin, J.,
- Shi, J.,
- Zhao, T.,
- Bai, J.,
- Li, J.
- and Zhou, W.
https://doi.org/10.1684/epd.2020.1230
Cite this article
- Liu, Y.,
- Wang, S.,
- Hong, B.,
- Wang, H.,
- Lin, J.,
- Shi, J.,
- Zhao, T.,
- Bai, J.,
- Li, J.
- and Zhou, W.
- Liu, Yiou.,
- et al.
- LIU, Yiou,
- WANG, Siyu,
- HONG, Bo,
- WANG, Haixiang,
- LIN, Jiuluan,
- SHI, Jie,
- ZHAO, Tong,
- BAI, Jianjun,
- LI, Jia
- and ZHOU, Wenjing,
https://doi.org/10.1684/epd.2020.1230
1 The orbitofrontal cortex (OFC), which rests on the roof of the orbit, is one of the least explored regions of the cerebral cortex (Geier et al., 1977; Chauvel et al., 1995; Niedermeyer et al., 1998; Bartolomei et al., 2000).
2 Epileptic seizures starting from the OFC have been less characterized in comparison with other types of epilepsy .The main reasons for the rare studies of medial OFE and lateral orbitofrontal epilepsy (OFE) may be the complexity of anatomical partition, rare cases, inaccessibility of this region to surface electrodes and the resulting need for invasive recordings. In a previous review reporting the largest number of OFE, only 32 cases could be established as OFE, which was based on the criteria of a lesion localized in the OFC or the patient being seizure-free after surgical removal of the OFC in cases of non-lesional OFE; these diagnostic criteria could be disputed. Chibane et al. also pointed out that further study is required to identify discriminative features between medial and lateral OFE (Chibane et al., 2017). OFC has vast bidirectional connectivity to a distributed network involving the frontal lobe, the temporal lobe, and the limbic system (Wang et al., 2013). Kriegel et al. reported that OFE presents with either frontal lobe type seizures or temporal lobe type seizures depending on the spread pattern (Kriegel et al., 2012), however, no specific area, representative of where these symptoms occur, was described. In humans, indeed in all primates, the posterior part of the OFC is connected with the anterior part of the insula (Cavada et al., 2000). Smith et al verified this by stimulating 13 posterior orbitofrontal sites and inducing a variety of sensations, which were mainly body tingling (Simith et al., 2004). Rostrally placed OFC blends into the dorsolateral part of the prefrontal cortex. However, no study has identified the discriminative features and connection between medial and lateral OFE. Moreover, outcomes of surgery in patients with epilepsy originating solely from the medial or lateral OFC remain uncertain. Lesions or damage to the OFC have been associated with significant changes in emotion, personality, behaviour, and social conduct. The most recent reports indicate that prefrontal seizures, particularly ventromedial seizures, are correlated with strong emotionality and vocalization with bilateral and symmetrical hyperkinetic movements, and the dorsolateral part may manifest as stereotyped hyperkinetic movements with moderate vegetative signs, speed, and vocalization (Fayerstein, 2020). Marseille's cluster analysis study elaborated on the symptomatology and related localization of frontal lobe seizures. Although the symptomatology of each representative region of the OFC was not presented, the study showed that the lateral orbitofrontal area (BA 47/12) may be associated with relatively integrated movement, such as distal stereotypies or manipulative behaviour, and the medial orbitofrontal area (BA 14, BA11) may be associated with feelings of fear/anxiety/rage and negative emotional expression (Bonini et al., 2014). This is possibly due to the interaction between the prefrontal lobe and temporal lobe, in particular, the ventromesial cortex such as the hippocampus and anterior cingulate region (Alberto, 2005; Fayerstein, 2020). A better understanding of the electroclinical features of medial and lateral OFE is therefore helpful for us to understand their characteristics and perform accurate resection, in order to protect the cognitive and behavioural functions of patients (Pereira et al., 2015). In this study, we selected cases in which seizures originated solely from medial or lateral OFC in order to explore electroclinical differences. In addition, epileptogenicity index and high-frequency oscillations (HFOs) were selected as the bio-electrical markers to demonstrate the seizure onset zone (SOz) and early propagation region.
Methods
3 Four patients who had undergone epilepsy surgery were enrolled at the Epilepsy Center of Yuquan Hospital Tsinghua University in Beijing. The epileptic foci in two patients originated from the lateral OFC and those in the other two from the medial OFC, which was confirmed by SEEG. We defined the lateral OFC as situated lateral to the lateral orbital sulcus and joined to the pars orbitalis of the inferior frontal gyrus, and defined the medial OFC as located within the medial orbital sulcus (Pereira et al., 2015). The gyrus rectus, which lies along the medial margin of the orbital lobe, was also classified as the medial part. Tailored resection or RF-TC guided by SEEG was performed on all patients. The patients underwent a comprehensive presurgical evaluation, including MRI, long-term video-EEG (VEEG), positron emission tomography (PET), and a neuropsychological test. MRI scans of three-dimensional (3D) T1-weighted 1.0-mm-thick contiguous slices, fluid-attenuated inversion recovery (FLAIR) sequences, double inversion recovery (DIR) sequences, and T2-weighted (2D, axial, and coronal) and FLAIR sequences (2D, axial and coronal) were obtained. SEEG was proposed to identify the EZ and better define a possible surgical resection limit. Between 6 and 16 electrodes with multiple contacts (10-15 contacts, length: 2 mm, diameter: 0.8 mm, 1.5 mm apart) were implanted per patient depending on the suspected origins in stereotactic conditions. Anatomical locations of the electrode leads were checked by the fusion of post-implantation CT with the reconstruction of the 3D image based on a preoperative T1-weighted MRI (Liu et al., 2019; Bai et al., 2019). Intracerebral recordings were performed using a video EEG system (Nihon-Kohden, Tokyo, Japan) with a sampling rate of 2,000 Hz. All seizures were reviewed by two independent reviewers.
4 Time-frequency spectrograms were also provided for assistance, which were calculated automatically by built-in software from Nihon Kohden. We used this measure to characterize epileptogenic activity and energy transfer. The presence of rapid discharges can be quantified after the transformation of raw SEEG signals (using a Morlet wavelet transform [MWT]) into the time-frequency plane around seizure onset; the baseline is automatically set to the beginning of the waveforms. Temporal spectral evolution (TSE) on a colour scale shows the amplitude and power change in each frequency band for each time period (Quyen et al., 2001). In order to visualize the high-frequency energy changes, we used Brainstorm to calculate the epileptogenicity index and presented high-frequency energy on the 3D brain (David, 2011; Tadel et al., 2011). The notion of the “epileptogenicity index” was first introduced by Bartolomei and was applied to SEEG signals to perform quantified studies of different types of seizures (Bartolomei et al., 2008). Our approach to the epileptogenic index is a modification of the methodology, but retaining the same philosophy.
5 We generated MWTs on a logarithmic scale, from 1 to 150 Hz, using the “flattening” option to amplify the higher frequencies and produce a more visually appealing image. A baseline of at least 20 s was chosen within the 2 min preceding the seizure, which needed to be void of any artifact. The baseline MWTs were used to normalize the seizure data of MWTs (Grinenko et al., 2018). We also superimposed the change in high-frequency energy on the 3D reconstructed brain with a colour code in order to more intuitively show the transfer of high-frequency energy as the seizure evolves. When several seizures were recorded in the same patient, all corresponding data could be pooled together to complete data analysis.
6 After the SEEG evaluation, patients underwent a tailored resection, or RF-TC of the identified epileptogenic zone. Postoperative MRI was acquired at least six months after surgery. Seizure outcomes were assessed by neurosurgeons according to the Engel scale.
Results
7 The clinical and SEEG data of four patients are displayed in table 1. A total of 21 predominantly sleep-related seizures were recorded.
| Lateral orbitofrontal | Medial orbitofrontal | |||
|---|---|---|---|---|
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | |
| Age at onset (y) | 6 | 8 | 2 | 11 |
| Age at SEEG (y) | 7 | 34 | 3 | 17 |
| Main semiology | Pelvic thrusting, pedalling, awareness | Pelvic thrusting, pedalling, awareness | Palpitations, manual and oral-facial automatism, impaired awareness | Attention impairment, manual and oral-facial automatism |
| MRI | normal | normal | normal | normal |
| PET (hypometabolism) | R-frontal | normal | L-frontotemporal | L-temporal |
| Interictal (scalp) | R-frontotemporal | R-anterior head | L-anterior head | Bil-anterior head |
| Onset (scalp) | R-frontal slow | none | anterior head Slow wave | L-temporal Sharp wave |
| No. electrodes (contacts) | 6 (94) right | 14 (200) 4 left, 10 right | 9 (140) left | 16 (236) 9 left, 7 right |
| Total seizure | 5 | 7 | 2 | 7 |
| Mean duration (s) | 21.17±11.5 * | 127.22±235.05 | ||
| Onset (SEEG visually) | LatOrG (R) | LatOrG (R) | Rectus gyrus (L) | Rectus gyrus (L) |
| epileptogenicity index positive zone (SEEG) | LatOrG (R) | LatOrG (R) | Rectus gyrus (L) | Rectus gyrus (L) |
| Early propagation area (SEEG) | SFS, IFG | MFG and trIFG | InsP, AM | InsP, TP, Hi, |
| Early propagation duration (s) | 7.92±4.44 * | 29.0±33.47 | ||
| Surgery/thermocoagulation | RF-TC of LatOrG (R) | RF-TC of LatOrG (R)→OFG (R) resection | Part resection of OFG (L) →rectus (L) | RF-TC of rectus (L) |
| Histopathology | NA | FCD IIb | FCD IIb | NA |
| Outcome (Engel)/FU (months) | Class IB (14) | Class IA (6) | Class IA (10) | Class IA (14) |
L: left; R: right; InsP: insular pole; AM: amygdala nuclei; OFG: orbitofrontal gyrus; Bil: bilateral; InsP: insular pole; TP: temporal pole; Hi: hippocampus; NA: not applicable; LatOrG: lateral orbital gyrus; SFS: superior frontal sulcus; IFG: inferior frontal gyrus; MFG: middle frontal gyrus; trIFG: pars triangularis; RF-TC: radiofrequency thermocoagulation. *p<0.05 (lateral orbitofrontal vs medial orbitofrontal).
Lateral OFE: Patients 1 and 2
8 Patients 1 and 2 had negative MRI images. Interictal discharges were limited to the anterior head. Hypometabolism on PET was found in the frontal area for one patient, and the other had no significant change; no hypometabolism in the temporal lobe was found in either patient. According to the scalp EEG, seizures arose from one side of the anterior head (Patient 1) or SOZ was unclear (Patient 2). Clinically, Patient 1 and Patient 2 had no symptoms at the beginning of the seizures, and then hypermotor symptoms appeared. When discharges propagated to the lateral part of the frontal lobe, the clinical manifestations of the two patients were extremely similar, beginning with pelvic thrusting, pedalling or raising of the legs; the manifestations were mild in Patient 1 and severe in Patient 2. Neither patient had a generalized tonic-clonic seizure. There were no significant vegetative neurological symptoms. Based on the SEEG, 12 clinical seizures from two patients were recorded with an average duration of 21.17 ± 11.5 s; both seizures started in the lateral OFC with low-voltage fast activities, then propagated to the lateral part of the frontal lobe, accompanied by hypermotor symptoms. The average duration of early propagation was 7.92 ± 4.44 s.
9 A time-frequency plane confirmed that high-frequency energy started earlier in the lateral OFC, followed by the lateral part of the frontal lobe, with Patient 1 propagating to the superior frontal sulcus and inferior frontal gyrus and Patient 2 propagating to the pars opercularis, middle frontal gyrus, and pars triangularis. This process was accompanied by delays or a decrease in frequency energy power. There was no high-frequency response in the temporal lobe (figure 1C, 2C). Epileptogenicity index analysis confirmed that the highest epileptogenicity index values for Patients 1 and 2 were in the lateral OFC (figure 1F, 2F). For Patient 1, dynamic high-frequency energy analysis of the 3D image showed early involvement of the lateral part of the OFC, followed by activation of the lateral part of the frontal lobe (2-3 s), after which energy increased when symptoms appeared (5-6 s) (figure 1D). For Patient 2, high-frequency oscillations originated from the lateral orbital gyrus, followed by the activation of the lateral part of the frontal lobe (12 s) and an increase of energy power in these areas (figure 2D).

LatOrG: lateral orbital gyrus; OFG: orbitofrontal gyri; SFS: superior frontal sulcus; IFG: inferior frontal gyrus; SOZ: seizure onset zone.
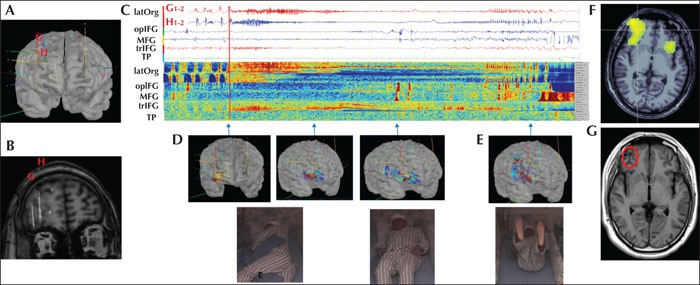
opIFG: pars opercularis; MFG: middle frontal gyrus; trIFG: pars triangularis.
10 RF-TC was performed for Patient 1 in the lateral OFC, and she had one simple partial seizure after 14 months. RF-TC was initially performed for Patient 2, and he was seizure-free for 12 months; when seizures recurred, he had right orbitofrontal lobe resection and had no seizures after six months of follow-up.
Medial OFE: Patients 3 and 4
11 The two patients had negative MRI images. Interictal discharges arose from one side or bilateral sides of the anterior head. Hypometabolism on FDG-PET was found in the frontotemporal lobe for one patient and in the temporal lobe for the other. Seizure onset was characterized by a slow wave or sharp discharges from one side of the anterior head. No specific aura was found. No symptoms were found at the beginning of the seizures. Symptoms appeared when discharges propagated to eloquent areas. Both patients showed the symptoms of medial temporal lobe epilepsy, including oral-facial and manual automatism, impaired awareness, and vegetative nervous symptoms such as palpitations and hyperventilation. Intracranial monitoring recorded nine clinical seizures with an average duration of 127.22 ± 235.05 s. SEEG indicated that both seizures started in the rectus gyrus with low-voltage fast activities, then propagated to the medial structure of the temporal lobe or insular lobe and showed symptoms associated with the limbic system (figure 3C, 4C). The average duration of early propagation was 29.0 ± 33.47 s. We defined the ipsilateral propagation time as the time elapsed from electrographic seizure onset to initial spread to an adjacent ipsilateral lobe.
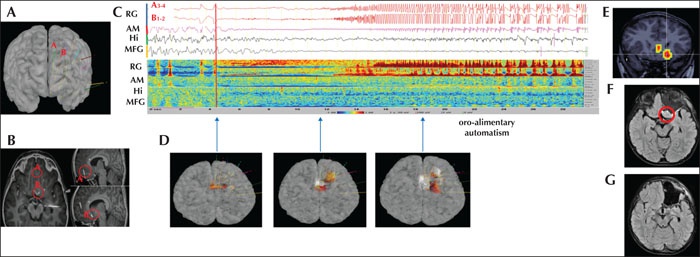
RG: rectus gyrus; postOrG: posterior orbital gyrus; InsP: insular pole; AM: amygdala nuclei; SFG: superior frontal gyrus.
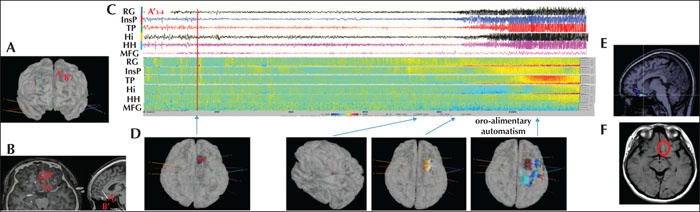
SFG: superior frontal gyrus; RG: rectus gyrus; InsP: insular pole; TP: temporal pole; Hi: hippocampus; HH: head of hippocampus.
12 High-frequency energy started earlier from the gyrus rectus, followed by the medial part of the temporal lobe, and in Patient 3 propagated to the amygdala nuclei and hippocampus, and Patient 4 to the insular pole, temporal pole, and hippocampus, as shown in the time-frequency plane (figure 3C, 4C). This process was accompanied by delays or a decrease in frequency energy power. There was no high-frequency response in the lateral part of the frontal lobe. Epileptogenicity index analysis confirmed that the highest epileptogenicity index value was in the rectus gyrus (figure 3E, 4E). High-frequency energy superimposed on the 3D image was highly successful in reconstructing high-frequency energy transfer, which showed early involvement of the medial orbitofrontal lobe, followed by energy activation of the medial temporal lobe (20 s) for Patient 3 and activation of the insular pole and temporal pole (60 s) for Patient 4 (figure 3D, 4D).
13 Patient 3 underwent two surgical resections. Part of the rectus was missed in the first resection, and he still had frequent seizures. The missed part was then removed in the second resective surgery, and he was seizure-free after 10 months, which confirmed the epileptic origin of the posterior gyrus rectus. RF-TC was performed on the left rectus gyrus of Patient 2, who was seizure-free after 14 months of follow-up.
Discussion
14 There have been few studies on the electroclinical characteristics of OFE due to the rarity of cases and difficult diagnosis. Description of the anatomical features of the OFC in humans is limited in the literature except for some functional studies involving the general area. A recent anatomical study in humans concluded that five gyri of OFC, namely the gyrus rectus, orbital medial gyrus, orbital anterior gyrus, orbital lateral gyrus, and orbital posterior gyrus, were delimited by four main sulci (Pereira et al., 2015). In most cases, however, the OFC is divided into the lateral, medial, and intermediate cortex by two longitudinal orbital sulci (orbital medial sulcus and orbital lateral sulcus). Therefore, the latter anatomical definition was used in the present study to differentiate the medial part of the OFC from the lateral part of the OFC. The gyrus rectus, which lies along the medial margin of the orbital lobe, is defined as the medial OFC (Jean et al., 2006). Both medial OFE and lateral OFE lack specificity in terms of scalp EEG. In general, interictal or ictal scalp EEG studies are not very helpful in identifying epileptogenic foci residing in the basal frontal lobe because of the hidden location of this part. Orbital discharges may have a regional distribution or appear generalized. In our four patients, the interictal discharges were confined to the anterior head, and the EEG changes at the onset could also be manifested in various forms. Interictal epileptiform discharges always allowed lateralization but not precise localization. Ictal scalp EEG recordings of OFE may provide poor localizing value, since false localization to the temporal region is not uncommon in patients with OFE, such as in Patient 4, whose scalp EEG showed temporal lobe origin, which may lead to false localization. PET identified hypometabolism extending outside the OFC. The medial temporal lobe structure showed low PET metabolism in medial OFE, which may be associated with propagation to the limbic system. However, PET hypometabolism was negative in the lateral OFE group or was confined to the frontal region without involving the medial temporal lobe, explaining the independent network of medial and lateral OFE.
15 The prefrontal cortex may be clinically silent, and seizures usually give rise to ictal manifestations by virtue of propagation to eloquent areas of the cortex. We observed this by using intracranial electrodes; when the seizure started from the OFC, there were no clinical symptoms. In addition, no secondary generalized seizures were found in either lateral OFE or medial OFE, indicating that OFE is less likely to cause GTCS. Frequent features of OFE include predominantly sleep-related seizure occurrence, lack of aura, and hypermotor manifestations such as automatisms and thrashing movements, which is consistent with our report. Some case series have reported sudden motion arrest and unresponsiveness at the beginning (Talairach, 1992; Munari, 1992). Previous literature has indicated that if discharges propagated rapidly from the OFC to the mesial temporal structures, déjà-vu feelings and oral-facial and manual automatisms were most prominent. Hence, OFE is electroclinically indistinguishable from temporal lobe seizures given the widespread connections between the limbic system and the OFC (Shihabuddin, 2001; Rheims et al., 2005). If it spreads to the dorsolateral frontal regions, hyperactive automatisms with frenetic, agitated movements prevail (Kriegel et al., 2012). We observed, through intracranial electrodes, that medial OFE propagated to the medial temporal lobe and insular lobe. The close relationship between the OFC and the limbic system has been well known; the uncinate fasciculus and the so-called ventral and dorsal limbic pathways are the main bidirectional association pathways linking the OFR with the temporal lobe, which explains the close connection between the two. In this study, the lateral part of the OFC propagated to the dorsolateral frontal lobe, and the symptoms were more rigid and movement was integrated. This appears to be more in line with Group 3 of the symptomatology identified by Bonini et al. (2014). At the same time, our intracranial electrode also confirmed that this specific manifestation occurred when the discharge propagated to the dorsolateral frontal lobe. Anatomically speaking, the anterior orbital gyrus and the rostral part of the lateral orbital gyrus are considered part of the middle frontal gyrus, which could explain the propagation from the lateral OFC to the dorsolateral part of the frontal lobe. It should be emphasized that this hyperkinetic behaviour is not necessarily limited to the dorsolateral frontal part. The repetitive nature of some hyperkinetic behaviour suggests the possibility of a similar mechanism which may occur in other clinical conditions. In this study, lateral OFE was shown to be more prone to this relatively integrated and unique movement, without frightened facial expression or screaming. This is more “cortical-dependent” than “subcortical-dependent”, since identical hyperkinetic behaviour could emerge from two distinct independent cortical networks (Bartolomei et al., 2005; Vaugier et al., 2009; Guedj et al., 2012; Vaugier et al., 2017).
16 In general, seizures arising from the frontal lobe may start and end abruptly and tend to have a shorter duration. Some investigators have observed that “orbitofrontal seizures” propagate more slowly, with a period ranging from 12.5 to 85 s, compared to seizures arising from other frontal regions (Munari et al., 1995). However, our study found that the duration of propagation of OFE depends on where the seizure started. The exact mechanism is unclear.
17 Two-dimensional (2D) and three-dimensional (3D) epileptogenicity maps, quantifying high-frequency oscillations (HFOs) at seizure onset, demonstrate good reproducibility and sensitivity and have proven helpful for better understanding the epileptogenic brain networks subserving different kinds of focal seizures (Coubes et al., 1993; Bartolomei et al., 2008; Blauwblomme et al., 2011; David et al., 2011; Job et al., 2014).
18 In ideal circumstances, the orbitofrontal origin of the epilepsy is deduced postoperatively on the basis of a surgical resection restricted to the OFC, leading to long-term cessation of seizures after surgery. Many of the reported cases of OFE were combined OFE and temporal lobe epilepsy cases, for which both regions were resected. Resection of the OFC alone is rare, let alone the distinction between medial and lateral OFE. Additionally, the inclusion criteria for OFE are controversial (Ludwig et al., 1975; Munari et al., 1995). All patients in our group underwent RF-TC or focal resection and achieved satisfactory results, which further supported the focal onset of seizure solely from the medial OFC and lateral OFC.
Limitations
19 We acknowledge that the number of cases in this study was small due to the restricted criteria. In addition, the medial OFE only covered the gyrus rectus, and did not include other structures medial to the orbital medial sulcus. In addition, the anterior orbital gyrus and posterior orbital gyrus should also be investigated, which requires more detailed research in this area.
Conclusion
20 In this study, we sought to obtain a better understanding of OFE, in particular, to distinguish the electrical electroclinical features and network between lateral orbitofrontal and medial OFE. The results show that medial OFE and lateral OFE are relatively independent with regards to clinical symptoms and epileptic networks. Moreover, scalp EEG and imaging are not specific, which could be misleading for surgery, therefore intracranial electrodes are needed to further clarify the seizure onset and define a precise resection area in order to protect the cognitive and behavioural functions of patients.
Disclosures
21 None of the authors have any conflict of interest to declare.
References
- Alberto Tassinari et al., 2005 Alberto Tassinari C., Tassi L., Calandra-Buonaura G., et al. Biting behavior, aggression, and seizures. Epilepsia 2005 ; 46 : 654-63.
- Bai et al., 2019 Bai J., Zhou W., Wang H., et al. Value of stereoelectroencephalography (SEEG)-guided radiofrequency thermocoagulation in treating drug-resistant focal epilepsy. Brain Sci Adv 2019 ; 5(3) : 189-202.
- Bartolomei and Chauvel, 2000. Bartolomei F, Chauvel P. Seizure symptoms and cerebral localisation: frontal lobe and rolandic seizures. In: Oxbury JM, Polkey CE, Duchowny M. Intractable Focal Epilepsy. WB Saunders, London, 2000; 55-62.
- Bartolomei et al., 2008 Bartolomei F., Chauvel P., Wendling F. Epileptogenicity of brain structures in human temporal lobe epilepsy: a quantified study from intracerebral EEG. Brain 2008 ; 131(7) : 1818-30.
- Bartolomei et al., 2005 Bartolomei F., Trébuchon A., Gavaret M., Régis J., Wendling F., Chauvel P. Acute alteration of emotional behaviour in epileptic seizures is related to transient desynchrony in emotion-regulation networks. Clin Neurophysiol 2005 ; 116(10) : 2473-9.
- Blauwblomme et al., 2011 Blauwblomme T., Kahane P., Minotti L., et al. Multimodal imaging reveals the role of activity in eating-reflex seizures. J Neurol 2011 ; 82(10) : 1171-3.
- Bonini et al., 2014 Bonini F., Mcgonigal A., Trébuchon A., et al. Frontal lobe seizures: from clinical semiology to localization. Epilepsia 2014 ; 55(2) : 264-77.
- Cavada, 2000. Cavada C. The anatomical connections of the macaque monkey orbitofrontal cortex. A review. Cerebral Cortex 2000 ; 10(3) : 220-42.
- Chauvel et al., 1995 Chauvel P., Kliemann F., Vignal J.P., et al. The clinical signs and symptoms of frontal lobe seizures. Phenomenology and classification. Adv Neurol 1995 ; 66(1) : 115-25.
- Chibane et al., 2017 Chibane I.S., Boucher O., Dubeau F., et al. Orbitofrontal epilepsy: case series and review of literature. Epilepsy Behav 2017
- Coubes et al., 1993 Coubes P., Awad L.A., Antar M., et al. Comparison and spacial correlation of interictal HMPAO-SPECT and FDG-PET in intractable temporal lobe epilepsy. Neurol Res 1993 ; 15(3) : 160-8.
- David et al., 2011 David O., Blauwblomme T., Job A.S., et al. Imaging the seizure onset zone with tereo-electroencephalography. Brain 2011 ; 134(10) : 2898-911.
- Fayerstein et al., 2020 Fayerstein J., McGonigal A., Pizzo F., et al. Quantitative analysis of hyperkinetic seizures and correlation with seizure onset zone. Epilepsia 2020 ; 61(5) : 1019-26.
- Geier et al., 1977 Geier S., Bancaud J., Talairach J., et al. The seizures of frontal lobe epilepsy. A study of clinical manifestations. Neurology 1977 ; 27(10) : 951-8.
- Grinenko et al., 2018 Grinenko O., Li J., Mosher J.C., et al. A fingerprint of the epileptogenic zone in human epilepsies. Brain 2018 ; 141(1) : 117-31.
- Guedj et al., 2012 Guedj E., McGonigal A., Vaugier L., Mundler O., Bartolomei F. Metabolic brain PET pattern underlying hyperkinetic seizures. Epilepsy Res 2012 ; 101(3) : 237-45.
- Job et al., 2014 Job A.S., De Palma L., Principe A., et al. The pivotal role of the supplementary motor area in startle epilepsy as demonstrated by SEEG epileptogenicity maps. Epilepsia 2014 ; 55(8) : e85-8.
- Kriegel et al., 2012 Kriegel M.F., Roberts D.W., Jobst B.C. Orbitofrontal and Insular Epilepsy. J Clin Neurophysiol 2012 ; 29(5) : 385-91.
- Ludwig, 1975. Ludwig B. Cerebral seizures of probable orbitofrontal origin. Epilepsia 1975 ; 16(1) : 141-58.
- Munari, 1992. Munari C. Electroclinical symptomatology of partial seizures of orbital frontal origin. Adv Neurol 1992 ; 57(2) : 257-65.
- Munari et al., 1995 Munari C., Tassi L., Di L.M., et al. Video-stereo-electroencephalographic investigation of orbitofrontal cortex. Ictal electroclinical patterns. Adv Neurol 1995 ; 66 : 273
- Niedermeyer, 1998. Niedermeyer E. Frontal lobe epilepsy: the next frontier. Clin Electroencephalogr 1998 ; 29
- Pereira et al., 2015 Pereira R.T., Silva R.M.A., Paz Daniel de Araújo, et al. Orbitofrontal sulcal and gyrus pattern in human: an anatomical study. Arq Neuropsiquiatr 2015 ; 73(5) : 431-44.
- Quyen et al., 2001 Quyen M.L.V., Foucher J., Lachaux J.P., et al. Comparison of Hilbert transform and wavelet methods for the analysis of neuronal synchrony. J Neurosci Methods 2001 ; 111(2) : 83-98.
- Rheims et al., 2005 Rheims S., Demarquay G., Isnard J., et al. Ipsilateral head deviation in frontal lobe seizures. Epilepsia 2005 ; 46(11) : 1750-3.
- Shihabuddin et al., 2001 Shihabuddin B., Abou-Khalil B., Delbeke D., et al. Orbito-frontal epilepsy masquerading as temporal lobe epilepsy: a case report. Seizure 2001 ; 10(2) : 134-8.
- Smith et al., 2004 Smith J.R., Sillay K., Winkder P., King D.K., Loring D.W. Orbitofrontal epilepsy: electroclinical analysis of surgical cases and literature review. Stereotact Funct Neurosurg 2004 ; 82(1) : 20-5.
- Tadel et al., 2011 Tadel F., Baillet S., Mosher J.C., John C., et al. Brainstorm: a user-friendly application for MEG/EEG analysis. Comput Intell Neurosci 2011
- Talairach et al., 1992 Talairach J., Bancaud J., Bonis A., et al. Surgical therapy for frontal epilepsies. Adv Neurol 1992 ; 57 : 707-32.
- Vaugier et al., 2009 Vaugier L., Aubert S., McGonigal A., et al. Neural networks underlying hyperkinetic seizures of “temporal lobe” origin. Epilepsy Res 2009 ; 86(2-3) : 200-8.
- Vaugier et al., 2017 Vaugier L., McGonigal A., Lagarde S., et al. Hyperkinetic motor seizures: a common semiology generated by two different cortical seizure origins. Epileptic Disord 2017 ; 19(3) : 362-6.
- Wang et al., 2013 Wang Z.I., Ristic A.J., Wong C.H., et al. Neuroimaging characteristics of MRI-negative orbitofrontal epilepsy with focus on voxel-based morphometric MRI post-processing. Epilepsia 2013 ; 54 : 12
- Liu and Zhou, 2019. Liu Y., Zhou W. Clinical features and surgical treatment of epilepsy after viral encephalitis. Brain Sci Adv 2019 ; 5(1) : 41-50.
Publisher keywords: high-frequency energy, lateral orbitofrontal epilepsy, medial orbitofrontal epilepsy, radiofrequency thermocoagulation (RF-TC), surgery
Uploaded: 09/16/2024
https://doi.org/10.1684/epd.2020.1230